









Sean’s story
Last week I introduced a case of overtraining syndrome (OTS) recovery strategy (not to be confused with an OTS case study) describing Sean’s story, my general approach and his first week of training.
The three-month strategy itself was designed according to certain choices about:
- Training session frequency
- Volume and intensity manipulation
- Monitoring through self-assessment and bloodwork
- Perceived exertion assessment method
- Pre-activation/warm-up
- Conditioning work
Training session frequency
We established four sessions per week according to his availability and our assessment of optimal stimulation at the time. Considering the general lack of consensus in the literature concerning OTS, the safe option was to use the minimum weekly volume and intensity that would keep him free of exercise-deprivation symptoms and move up from there. It seemed logical to distribute exercise sessions along the week with at least 48h between them.
Volume intensity manipulation
After negotiating with Sean what would be the most pleasant or fun exercises, I designed a strategy according to the following guidelines, in this order:
- Fun exercises
- Not more than 5 exercises including very simple prehab/rehab ones
- Short conditioning session after the core training exercises
- Low volume and low intensity at each session
Monitoring through self-assessment and bloodwork
Sean started feeling better after the first week. This was not a result of the training strategy alone and at this point, pharmacological treatment was probably the chief factor in his recovery. He provided us with feedback on an almost daily basis and the three of us (Sean, Walt and I) concluded that self-assessment was an important item of the program. This is not exactly original and you can read something about it here and here .
Perceived exertion assessment method
This is never easy to discuss outside academic circles given the quasi-religious approaches adopted in training by coaches, pseudo-coaches, and athletes. I have my own method that integrates a percentage prescription and perceived exertion through reps-in-stock. This is the subject for a long review and this is not the space for that. Feel free to browse part of my library on the subject.
Pre-activation / warm-up
Another controversial item. Sean is not a young athlete (early 40s) and he has accumulated several injuries throughout his athletic career. Pre-activation and warm-up become increasingly important in this class of athletes not only because there are several tissue scars (vulnerable to re-injury) but because the ability of these athletes to recover their strength and power output is higher than the rate at which we manage to recover them from damage.
Conditioning work
And yet another controversial item: as a coach, I believe every athlete must have a minimal level of conditioning. There are too many reasons for that, including tissue-level adaptations that favor recovery. Since Sean had been a Crossfit athlete for five years at that time, all I did was create short conditioning circuits that looked like the WODs he was familiar with.
The split
We adopted this simple split to be completed in a seven-day period (weekly cycle). Sean chose to favor powerlifting and bodybuilding exercises over Olympic weightlifting and odd objects at this time.
| Day | Main exercise | Assistance 1 | Assistance 2 |
| 1 | Pressing (benching, overheads) | Rows | Curls and forearm work |
| 2 | Squat and pulls | Clean and jerk | RDL, HGR, other hamstring work |
| 3 | Bench press | Single joint exercises | |
| 4 | Deadlift | snatch |
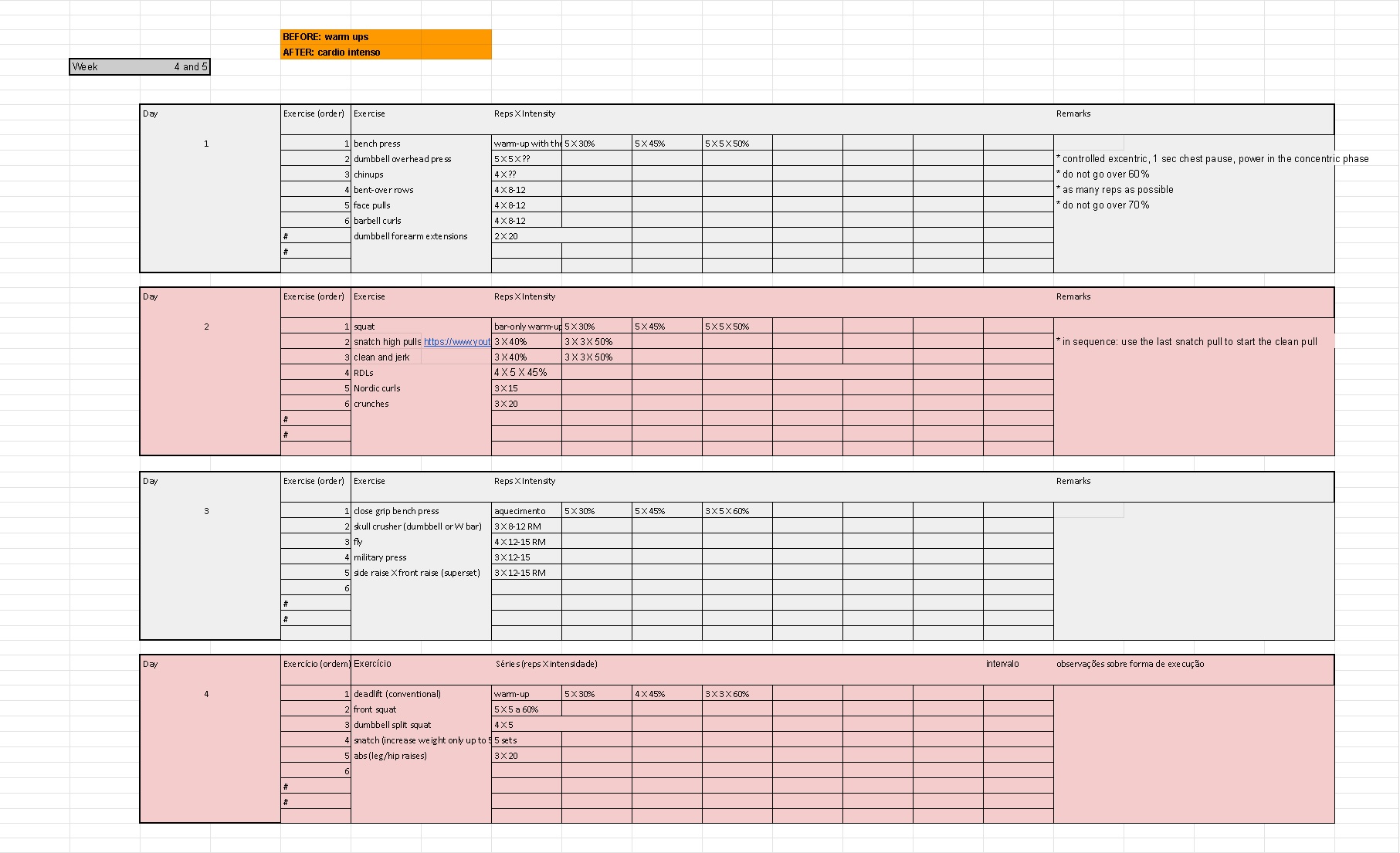
Sean’s 4thand 5th weeks:
https://bmcsportsscimedrehabil.biomedcentral.com/articles/10.1186/s13102-017-0079-8
Sports physicians will look at inflammatory indicators but this, too, is controversial. We do know that the HPA axis is affected:
https://sportsmedicine-open.springeropen.com/articles/10.1186/s40798-017-0113-0
Some physicians will look into CK levels (at base level, 24 and 72h after training) as a parameter, which I disagree, given the ample evidence of healthy variation in the medical literature.
Everyone will measure cortisol, GH and ACTH.
Both my partners (physicians) interpret bloodwork in the context of complex clinical evaluations. They mean very little out of context.