










In recent months I’ve seen the following phrase parroted: “breathing is bracing." I have also seen a number of Facebook or Instagram videos describing good bracing techniques while then describing diaphragmatic breathing. Don’t get me wrong; breathing properly is of critical importance and is the absolute first thing I address. If you have breathing dysfunctions, there is nearly an endless list of problems that can and will develop. Additionally, if you have dysfunction with one function of the diaphragm, such as breathing, you will have dysfunction with bracing.
But breathing and bracing, while integrated, are different. There are three functions to the diaphragm.
- Respiration
- Stabilization
- Sphincter
Once breathing (respiration) issues have been addressed with diaphragmatic breathing principals you can then move to stabilization. Before addressing actual stabilization approaches, one must first address posture. Without proper posture, stabilization will not work effectively.
WATCH: Physical Therapy — Anterior Pelvic Tilt Fix with Dani Overcash
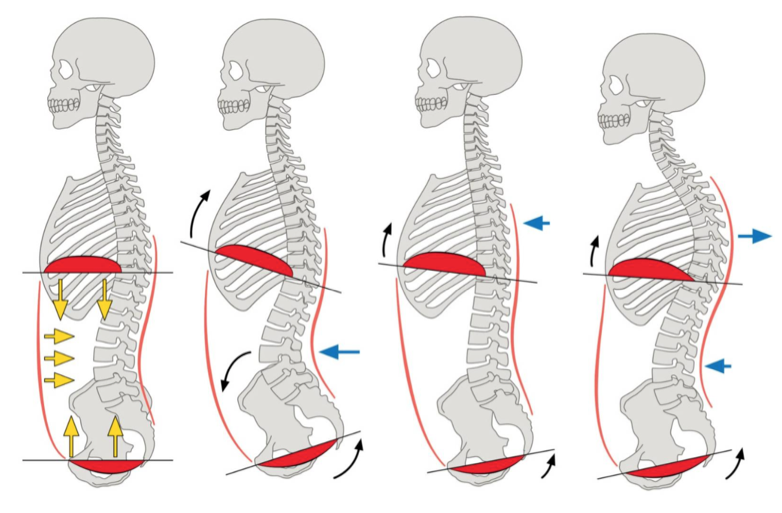
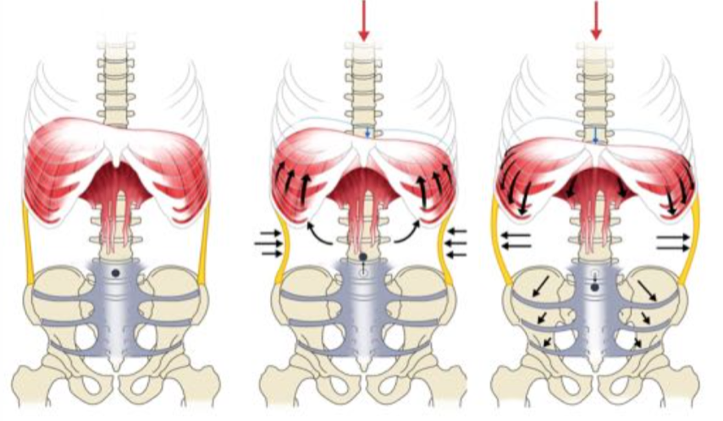
Below you can see different postures with the correct one being on the far left where the diaphragm (top) is working directly in opposition of the pelvic floor (bottom). This is where pelvic tilt and chest position need to be addressed.
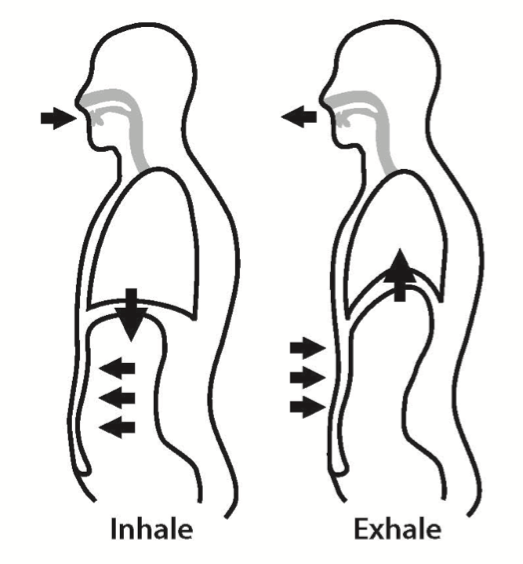
Many people who teach breathing as bracing have encountered a fatal flaw: air is not the stabilizing force. Yes, it is used to transmit force, but a big belly full of air is not bracing. And particularly, a big belly full of air towards the front such as yoga breathing is even worse. The picture below describing yoga breathing is not what we are going for in the stabilization function. It is even arguably wrong for respiration function as well.
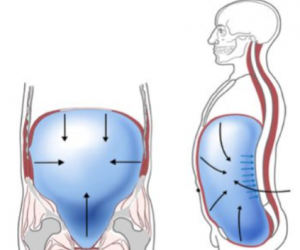
One must begin to think of a giant ball in the abdominal cavity and the force is going outwards in all directions with the same pressure. But in the bracing function, the pressure being generated between the diaphragm and pelvic floor that is being transmitted equally outward must be resisted. The outer sheath of the abdominal cavity resists that outward force.

While the air is transmitting the force, just having a giant belly full of air is not bracing. These equal and opposite forces pushing against each other generate the stabilization function. The importance of posture once again must be brought up; if the pelvic floor and diaphragm are not working directly in opposition of one another, there will be a leak out the front or back. Commonly the leak is out the front with either a raised chest or anterior pelvic tilt. This is called an open scissor and will result in less pressuring being forced towards the organs and low back, often resulting in comprised lumbar positioning during a lift.
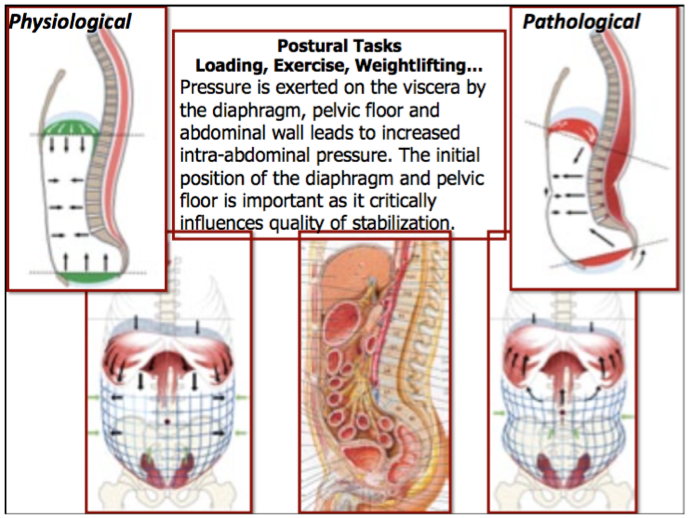
One of the assessments we look at is simply the shape of the abdominal region in relaxed, pressurized, and stabilized conditions. Hypertonic muscles in some areas, divots, and an overall any lack of conformity are indicators of some negative pathology.
On the left is a normal relaxed condition. In the middle is incorrect pressurization. Unfortunately, this is the "desired" hourglass figure people often go for, with clean, evident oblique lines and a tight belly. This is one reason I hate core work that is not focused on quality intra-abdominal pressurization. It reinforces the disconnect between the outer abdominal sheath and the diaphragm's stabilization function. It reinforces pathological patterns that break down stabilization functions. On the right is the correct pressurized condition.
Think about it as blowing up a hot water balloon vs. a balloon for a kid’s party. You want the hot water balloon for stabilization — a tight and restrictive outside sheath working against the air inside. That party balloon may have as much air in it, but it will deform as soon as apply pressure to any point to it. Don’t end up looking like this while you lift.
Now let's briefly touch on the integration of the respiration and stabilization functions, as well as one of the most infuriating questions I get. Recently I’ve been interviewed for a couple well-known fitness magazines by authors who have “read and watched all my content." One of the main questions I've received is, “When should someone breath while lifting? On the eccentric, between reps, or every few reps?” Good thing they were phone interviews so I could not strangle them.
IT DEPENDS! If one is doing a max lift, 5RM, 20 reps, MetCon, or marathon, the breathing is different. There are different levels of respiration and stabilization required for each of these and it operates on a continuum. If you're running a marathon, respiration is paramount and stabilizing very low. If squatting 1000 pounds, you are all stabilization and respiration takes a back seat. It could be any of the answers from breathing between every rep, breathing during reps, breathing every few reps, or not breathing at all. Think of it as a dial on a continuum with the marathon on the far left and breathing on the far right.
This article touches on the surface level of the concepts but should shape a good understanding of the fundamentals of the respiration and stabilization functions of the diaphragm. I hope to expand on this in future more in-depth articles and videos.
A big thanks goes out to all the DNS instructors I have worked with over the last four years from the Prague School of Medicine.
Images courtesy of Prague School of Medicine

or
"Think of it as a dial on a continuum with the marathon on the far left and bracing on the far right."