




Female urination in the weight room or on the platform has become a hot topic in many online communities. This type of urination is labeled as Urinary Incontinence (UI). UI is the involuntary loss of urine, which can happen in both males and females. (1) The percentage of women experiencing UI ranges from 10-55%. That is a pretty large range if you ask me! Hypothesizing that more than half of the female population experiences UI makes it seem like a common issue.
In athletics, the term changes from UI to SUI (stress urinary incontinence). Stress being placed on the pelvic floor, such as a cough, sneeze, or bracing, can cause SUI to occur. According to the data, the prevalence of SUI in the athletic population increases up to 80%, with an average of 49% (8). (3) The term "athletic incontinence" or "AI" is becoming common but it has not yet been accepted by the medical community. It is a term used to describe incontinence that occurs only when performing athletic activities. I will use these terms throughout this article.
Why Am I Writing This?
I am an elite powerlifter. I have totaled 1,334 pounds in competition at 164 pounds bodyweight. I am also a doctor of physical therapy. Although I do not suffer from AI, I know and have many close friends who do experience AI. I am also a gym owner, and I aim to provide a safe space for women who may or may not have AI. Although incredibly common, I understand involuntary urination is not considered a normal bodily function. With that being said, it does not mean it needs to be stigmatized, fixed, or "cured" each and every time it happens. Just because AI is not "normal" doesn't mean it's wrong. Being seven feet tall is not "normal," and it also is not wrong.
My quest to find answers beyond what is generally available about AI started in February 2022. I made a post on Instagram about elite-level lifters and the stress that the physical load places on the body while lifting weights. This outside stress and the amount of weight being lifted relative to one's body weight will overstress even the strongest of pelvic floor muscles at times. I received a lot of support on this post, but I also received a lot of backlash from pelvic floor therapists who claim, "any urination while lifting is not normal." I disagree with this on both practical and anatomical levels.
Survey Results
I conducted a survey online about UI that had 158 female participants. Twenty five percent of the women surveyed have stopped competing or weight lifting because of AI. Many of the comments noted about UI stopping females from doing activities in their sport or life deal with anxiety related to urination, specifically from what others will say or do, or the judgment passed onto them. One participant had her gym membership revoked due to her experiencing AI while lifting at the facility.
Data analysis shows an average of at what percentage of their 1-rep max women begin to experience AI in the squat and deadlift:
- 84% of 1-rep max for squat
- 83% of 1-rep max for deadlift
Further findings disclosed more women pee during conventional deadlift vs. sumo deadlift. This is due to the decreased inherent risk of lumbar flexion in sumo vs. conventional stance. Many women stated they experience leakage at lighter weights or earlier than normal when ovulating or when on their period. This is directly linked to the uterine lining thickening.
The devastation and stigma many women in particular feel from other people inserting their opinions on AI is disheartening. There are mitigating protocols one can employ, such as: voiding before each set, stimulating a void via urinary reflex contraction, wearing a pad or incontinence garment, or wearing darker clothing. But not all women will want to perform these tasks. It is not the opinion of the online judge and jury to decide the fate of someone suffering from SUI. It is a personal journey that should be left at that. PERSONAL. It is not a show that a woman is trying to put on, it is an involuntary action that is caused by stress placed on the PFM.
In my survey, I asked the participants to share what hurts them the most about AI.
- 90% wished people would understand how common an issue this is and wished it was less stigmatized.
- 74% are embarrassed about it. The general consensus of the women surveyed is women want people to realize this does not mean there is something wrong with them, they do not do it on purpose and this is not something done for attention.
- The biggest frustration expressed by the survey participants is they have a hard time focusing on their actual lifts when they are experiencing AI. The preoccupation with smell, visible stains, puddles, and glaring eyes from around the gym take up more mental space than a lifter has to be able to perform the rest of the workout after AI has occurred.
- 52% experience AI and do not wear any type of protective garments while lifting; 44% wear pads while lifting; 8% wear a diaper while lifting.
Limitations in the literature: there are no studies of elite level powerlifters that assess pelvic floor pressure while performing powerlifting movements. There are many surveys and studies done on lifters in the novice and intermediate categories. The best study I could find of 480 women had the highest total of 880 pounds which is incredible but not replicative of an entire group (elite and ultra elite) of AI lifters. There are other factors that can contribute to UI and AI, which include but are not limited to: childbirth, age-related changes, uterine prolapse, nutrient deficiencies, hysterectomies, abdominal surgeries, and bladder infections.
Practical Approach
The muscles of the pelvic floor are not the same size or density, nor do they possess the same cross sectional muscle fibers larger muscle groups like the lats or quadriceps do. Incontinence during physical stress is common in young, highly fit women. This suggests there is a continence threshold, which, when exceeded, can result in urine loss in some individuals, even in the absence of known risk factors for incontinence. (9)
Muscular fatigue is a real thing. Let's examine a powerlifter's typical training day. Your working weight is 85% of your max weight for four sets of three repetitions. Right there is 12 repetitions. It may take you up to 20 repetitions to get up to your working weight, or more. After 32+ repetitions, one would expect some muscular fatigue. If the pelvic floor muscles (PFM) are contracting during each repetition to hold the urine of the bladder, over time, there will be some pelvic floor "form breakdown."
Anatomical Approach
There are several factors that can cause extra pressure on the abdominal cavity, including the bladder.
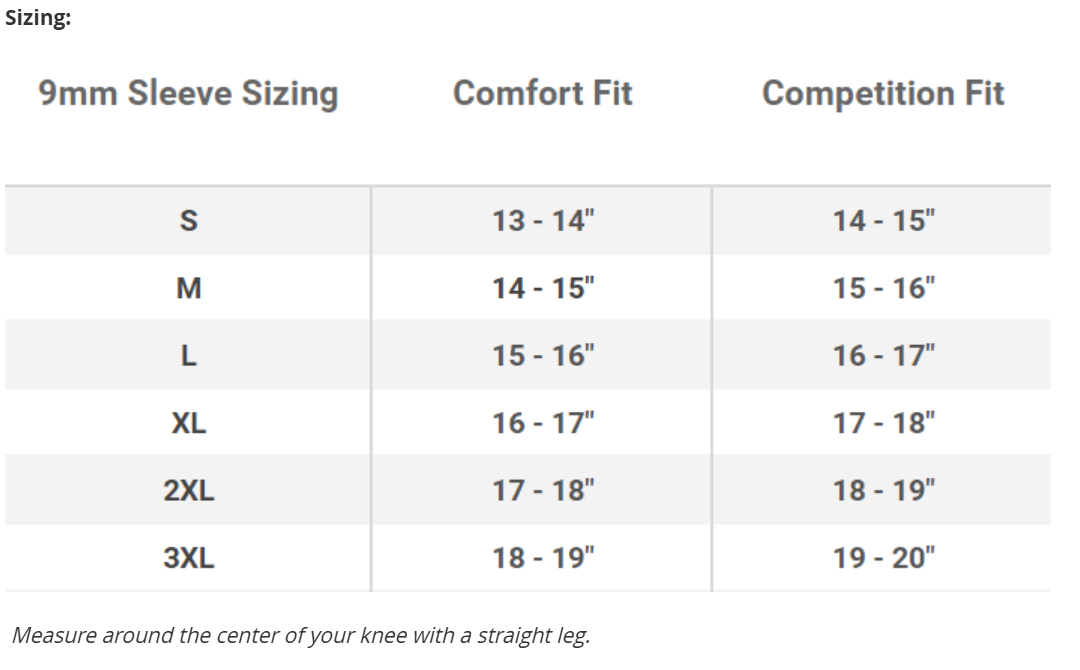
- Belt placement and usage. Belts come in a variety of shapes and sizes, from two inches in diameter to four inches. The thickness typically ranges from eight millimeters to 13 millimeters. The type of belt a lifter wears can anatomically change the intra-abdominal pressure placed on the lifter more than bracing alone can throughout the lift.
- Improper bracing can descend the pelvic floor and promote downward pressure that can promote voiding (a partial or full emptying of the bladder).
- Anatomical changes under load can change the relation of your torso to your gut and can cause pressure directly on the bladder, which can stimulate a voiding reflex. (4)
- Menstrual influences can change the size of the uterus and create increased pressure due to the uterine lining thickening. (4)
- Bloating or constipation can also increase intra-abdominal pressure.
I want to break down what I am referring to when I talk about spinal position eliciting a voiding reflex. There are complex systems our bodies use to regulate bodily functions. The one specific to urination is called the micturition reflex. The micturition reflex is one of the autonomic reflexes.
The release of urine is regulated by voluntary and involuntary mechanisms that involve centers in the brain and spinal cord. (5) The autonomic nervous system is a control system that acts largely unconsciously and regulates bodily functions. (6) The bladder has stretch receptors inside that when functioning normally, stretch when the bladder is full and send a signal to the brain telling your body, "it's time to go pee!" To urinate, it takes a conscious effort on your brain to allow your urinary sphincter to relax for the flow of urine to occur via the micturition reflex.
When squatting or deadlifting, it is easy to create increased pressure so quickly by descending in the squat or bending down to reach the bar, that your brain and body don't have time to communicate and the micturition reflex is stimulated without the brain's input to say, "Ok, we are ready for this to happen." Hence, pee pee in the squat and deadlift.
The deadlift has the highest occurrence for urination, followed by squat, then a very low percentage for bench. Studies show there is more intraabdominal pressure in the squat over the deadlift. (7) The position of the lumbar spine, however, is much more likely to flex in deadlift than squat. The deadlift is the most taxing lift on the body and central nervous system and, as previously stated, form breakdown is a contributing factor to AI.
When to Seek Help
I do want to point out there are instances where AI/SUI is not normal and should be assessed and corrected by a healthcare professional (specifically pelvic floor physical therapist). Pelvic floor physical therapists are physical therapists with specialized training to deal with issues in incontinence, pelvic pain, pregnancy, and other diagnoses that affect the pelvis. They treat both men and women who have pelvic-related problems. (10) If you have UI outside the gym or feel you would like to strengthen your PFM, just like any other muscle, it is definitely worth a few sessions to see if you are able to reduce your leakage or AI/SUI. It is concluded that PFM exercises are effective in treating SUI.
Self-reported cure and success rates of SUI when working with a specialist vary between 17% and 84%. They are cost-effective and should be the first choice of treatment. To be effective, PFM exercise has to be thoroughly taught and performed with weekly or monthly follow-ups. (11).
Some key signs and symptoms of when to seek out help:
- If you experience UI while outside the gym performing daily activities or when coughing, sneezing or laughing.
- If you experience SUI while jumping, either from the ground or on a trampoline.
- If you experience SUI with little to no load on the bar (<65% of your 1RM).
- If you experience SUI when wearing a belt but no SUI without a belt (this type of SUI is most likely linked to improper bracing).
- If you can feel a link with your fatigue level and SUI (you would most likely benefit from increased PFM strengthening).
- If you are coming back to lifting postpartum and your SUI has significantly changed (this can develop from stretching of the PFM and you would benefit from PFM strengthening).
Final Thoughts
I have discussed the practical and anatomical limitations of the PFM's ability to hold urine while weight lifting. I have explained when AI and SUI should be addressed by a clinician. I am now going to address a third and final point of view.
WHO GIVES A FUCK?! Really, who? I bet I could walk through any weight room in the country and find all of these things: 1) weakness 2) improper form 3) poorly fitted or wrong lifting equipment 4) form breakdown 5) misuse of equipment. These issues are common in any exercise and individuals and aren't just applicable to the expulsion of urine.
This attitude can be applied to any and all forms of lifting weights. You don't typically see online haters going off about a strict bicep curl vs. using momentum like you do when someone sees some urine on the platform. Neither of these are outright intentional, they just happen; through whatever mechanism, they just do. There are numerous people who exercise and lift weights who are fully aware of tightness, weakness, and pain they have in their bodies at rest and while lifting. It is their choice if and when they want to see a professional for help.
Why do so many pelvic floor therapists and online trolls feel the need to give unsolicited advice to a lifter about their perception of that lifter's AI-SUI? There aren't just two sides to this fence. A lifter isn't just incontinent or not. There are, shall we say, 50 shades of yellow? If someone wants to reach out and get help, that is on them. For now, can we just let pee pee be?
References
- ICS Glossary [Internet]. 2021 [cited 2 Nov 2021]. https://www.ics.org/glossary.
- Committee 1 Epidemiology of urinary incontinence and other lower urinary tract symptoms pelvic organ prolapse and anal incontinence. Epidemiology of urinary incontinence in women. In: Abrams P, Cardoso L, Wagg A, Wein A, editors. Incontinence. 6 ed. Bristol UK: ICI-ICS. International Continence Society; 2017. p. 17–35.
- Bø, K. Urinary Incontinence, Pelvic Floor Dysfunction, Exercise and Sport. Sports Med 34, 451–464 (2004).
https://doi.org/10.2165/00007256-200434070-00004 - Dr. Rori Alter. (2020, July 25). 3 REASONS YOU PEE WHEN YOU POWERLIFT & HOW TO FIX IT (PART 2): MECHANICAL CONTRIBUTION. Progressive Rehab and Strength. Retrieved March 22, 2022, from https://www.progressiverehabandstrength.com/articles/urinary-incontinence-powerlifting-part-2
-
Kuru, M. (1965). Nervous control of micturition. Physiol. Rev. 45: 425-494. - Schmidt, A; Thews, G (1989). "Autonomic Nervous System". In Janig, W (ed.). Human Physiology (2 ed.). New York, NY: Springer-Verlag. pp. 333–370.
- Blazek D, Stastny P, Maszczyk A, Krawczyk M, Matykiewicz P, Petr M. Systematic review of intra-abdominal and intrathoracic pressures initiated by the Valsalva manoeuvre during high-intensity resistance exercises. Biol Sport. 2019;36(4):373-386. doi:10.5114/biolsport.2019.88759
- Rebullido TR, Gómez-Tomás C, Faigenbaum AD, Chulvi-Medrano I. The Prevalence of Urinary Incontinence among Adolescent Female Athletes: A Systematic Review. Journal of Functional Morphology and Kinesiology. 2021; 6(1):12. https://doi.org/10.3390/jfmk6010012
- Nygaard IE, Thompson FL, Svengalis SL, Albright JP. Urinary incontinence in elite nulliparous athletes. Obstetrics and Gynecology. 1994 Aug;84(2):183-187. PMID: 8041527.
- Women's Health & Pelvic Floor therapy. Women's Health & Pelvic Floor Therapy | UI Health. (n.d.). Retrieved March 28, 2022, from https://hospital.uillinois.edu/primary-and-specialty-care/rehabilitation-services/physical-therapy/womens-health
- Bø, K. Pelvic floor muscle exercise for the treatment of stress urinary incontinence: An exercise physiology perspective. Int Urogynecol J 6, 282–291 (1995). https://doi.org/10.1007/BF01901527

Dr. Ashley Contorno is a board certified doctor of physical therapy with a private practice based inside of her gym, South Bay strength company, located in Los Angeles. She is an International Elite Powerlifter who holds the 2nd best bench in the world as a 75kg lifter. Dr. Ashley is passionate about education and passing on what she has learned as a coach, athlete, and gym owner.